Over the past months, we have released a number of posts introducing inhibitor screening assays intended to investigate immuno checkpoint protein interactions, such as PD-1/PD-L1/PD-L2; B7-1/CD28, B7-1/CTLA4; BLTA/HVEM, CD47/SIRPα; GITR/GITRL and many others – for an overview, you might like to read 9 pathway-specific screening assays in Immunotherapy.
Today, I’d like to concentrate on the TIGIT/CD226 pathway, because it acts through a novel mechanism to regulate CD8+ T cell functions within the tumour microenvironment.
The TIGIT/CD226 pathway parallels the CD28/CTLA-4 pathway that we covered in Immunotherapy Screening – B7-1 / CD28 and B7-1 / CTLA4 Pathways in Drug Discovery. Similar to CD28 and CTLA-4, CD226 and TIGIT share ligands, CD155 (also known as the poliovirus receptor, PVR) and CD112 (Nectin-2). CD226 and TIGIT (also known as VSTM3) can compete for ligand binding on target cells. However, CD226 and TIGIT binding have opposite results: whilst engagement of CD226 with CD155 or CD112 enhances T cell activation, the interaction between TIGIT and CD155 or CD112 inhibits T cell responses.
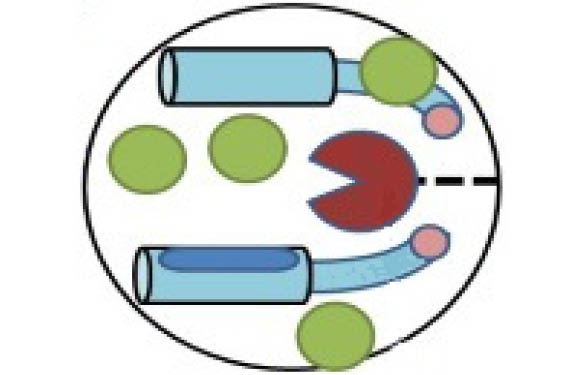
Both CD155 and CD112 are found on dendritic cells (DC) and macrophages, and both are highly overexpressed on multiple cancer cell lines and primary tumours. CD226 (also called DNAM-1) is expressed primarily on NK cells and CD8+ T cells. The CD226 glycoprotein acts as a co-stimulatory adhesion molecule, promoting Th1 differentiation, and triggering NK activation. Interactions between CD226 and the CD155/CD112 ligands play an important role in T cell and natural killer (NK) cell–mediated recognition and lysis of tumor cells (see Fig 1).
On the other hand, CD155/CD112 binding to TIGIT (T-cell immunoreceptor with immunoglobulin and ITIM domains) directly suppresses the cytolytic activity of NK cells and inhibits T cell proliferation and cytokine production in CD4+ T cells. TIGIT also indirectly inhibits T cell responses by triggering CD155 in DCs, thereby preventing DC maturation and inducing production of immuno-suppressive cytokines such as IL-10. Additionally, TIGIT has been shown to inhibit pro-inflammatory Th1 and Th17 responses. TIGIT can even physically block the dimerization of CD226, which prevents its co-stimulatory function.
Development of therapeutic antibodies
Not surprisingly, researchers are actively developing therapeutic monoclonal antibodies to regulate these pathways. Neutralizing the TIGIT pathway is especially promising because it blocks the negative TIGIT inhibitory signal on effector T cells while simultaneously promoting the positive CD226 stimulatory signals for T cell proliferation and pro-inflammatory cytokine production [IFN-γ, IL-17, IL-9], leading to T cell activation. Antibodies that block TIGIT binding to CD155 have been shown to prevent TIGIT’s down-regulation of NK cytotoxicity , and to decrease tumour growth. Similarly, an anti-CD112 monoclonal has been show to exert an in vivo anti-tumour effect on breast and ovarian cancer cells, which suggests the potential of CD112 as a target for antibody therapy for cancer treatment.
TIGIT expression is strongly associated with expression of other co-inhibitory molecules; PD-1, Tim-3 and Lag-3. Thus, many researchers are investigating combinations of blocking antibodies. Antibody blockade of the TIGIT pathway synergizes with Tim-3 blockade to maximally decrease tumour growth. Likewise, blockade of TIGIT signaling has been shown to synergize with PD-1/PD-L1 blockade to enhance antitumour CD8+ T cell responses in both humans and mice. In particular, antibody co-blockade of TIGIT and PD-L1 results in significant tumour clearance, and elicits tumour rejection in pre-clinical models.
Role of CD226/TIGIT in autoimmune and inflammatory diseases
In addition to cancer, the CD226/TIGIT pathway has been linked to several auto-immune and inflammatory diseases. For example, TIGIT engagement has been shown to ameliorate collagen-induced arthritis, while down-regulation of TIGIT exacerbates experimental auto-immune encephalomyelitis. CD226 binding to CD155 has been associated with auto-immune-linked disorders, including multiple sclerosis and type 1 diabetes, and treatment with a neutralizing anti-CD226 monoclonal efficiently inhibits activation and proliferation of T cells from patients with auto-immune diseases. Even better, naive T cells do not express CD226, so therapeutic strategies targeting CD226 would exclusively target pro-inflammatory Th1 and Th17 cells.

Overall, targeting the CD226/TIGIT pathway may provide a therapeutic approach that can modulate the pro-inflammatory and anti-inflammatory balance in a wide range of diseases.
Available tools for inhibitor screenings
To enable you to screen for the identification of small molecule inhibitors and antibodies that block receptor-ligand interaction using AlphaScreen technology, BPS Biosciences provides developed 4 unique kits for investigating the CD226/TIGIT pathway. Figure 2 shows results obtained with the TIGIT: CD155 Inhibitor Screening Assay Kit. Furthermore they offer the individual biotinylated and unlabeled proteins.
- TIGIT:CD112 Homogeneous Assay Kit
- TIGIT:CD155 Homogeneous Assay Kit
- CD226:CD112 Homogeneous Assay Kit
- CD226:CD155 Homogeneous Assay Kit
Any questions or comments? Please feel free to contact me with the form below!
 Interested in learning more about tools like this?
Interested in learning more about tools like this?Subscribe to thematic newsletters on your favourite research topics.